Essential Guide to Status Epilepticus Management PDF
Status Epilepticus Management Pdf serves as a vital resource for healthcare professionals navigating one of the most urgent neurological emergencies. Effective intervention within the first few minutes can mean the difference between recovery and long-term neurological damage. This essential guide explores every critical step, from initial recognition to post-epileptic care, grounded in current clinical evidence and presented through a comprehensive PDF format designed for quick reference and deep learning.
Understanding Status Epilepticus: Beyond the Basics
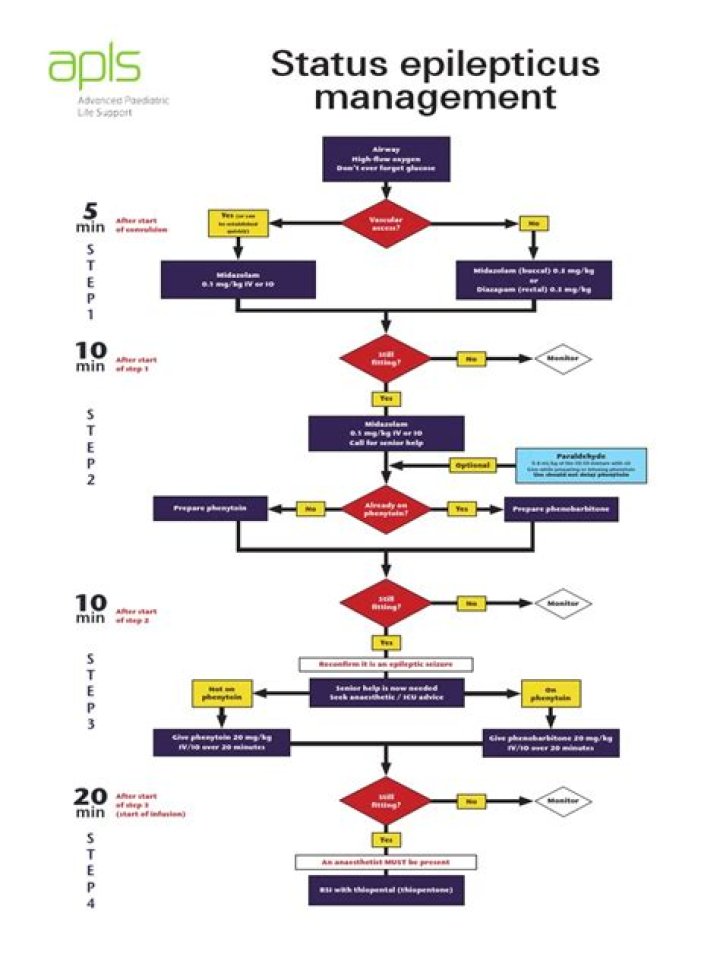
Understanding Status Epilepticus Management Pdf begins with recognizing its complexity—this is not a single event but a dynamic state demanding rapid, coordinated action. It refers to continuous seizure activity or repeated seizures without regaining consciousness, often triggered by metabolic disturbances, brain injury, infections, or drug toxicity. Every second counts; delays risk irreversible brain injury. A well-structured PDF resource breaks down pathophysiology, classification systems like focal vs generalized tonic-clonic epilepticus, and the urgent need for immediate stabilization before diving into treatment algorithms. When evaluating a patient in status epilepticus, distinguishing between continuous seizure and recurrent partial seizures guides initial management. The PDF emphasizes assessing airway protection, oxygenation, intravenous access, and avoiding hypoxia—foundational yet non-negotiable steps. Delayed oxygenation or inadequate sedation can escalate intracranial pressure rapidly, worsening outcomes. This guide reinforces that time is both a clinical parameter and a therapeutic tool in Status Epilepticus Management Pdf. The initial phase prioritizes airway management with early intubation if needed—especially when gag reflex is absent or respiratory compromise develops. Airway adjuncts serve as bridges while sedatives take effect; yet prolonged supine positioning risks aspiration pneumonias. Continuous monitoring of vital signs alongside EEG confirmation confirms seizure persistence even if clinical signs wane—highlighting why real-time data integration remains central in modern protocols detailed here.
Core Interventions: From Benzodiazepines to Advanced Therapies
Once the crisis stabilizes enough for controlled drug delivery, benzodiazepines anchor first-line treatment—lorazepam preferred due to rapid onset and longer duration compared to diazepam. These agents rapidly suppress neuronal hyperexcitability by enhancing GABAergic inhibition. The PDF outlines dosing regimens tailored to adult and pediatric populations while stressing vigilance against hypotension or respiratory depression during administration. If seizures persist beyond 5 minutes—classic Definition of Status Epilepticus—the next tier includes second-line agents such as fosphenytoin or midazolam via bolus or continuous infusion under strict hemodynamic monitoring. The document stresses that prolonged use of certain antiseizure medications may carry neurotoxic risks; thus timed escalation guided by response patterns is essential. In refractory cases where seizures resist standard therapies despite optimal supportive care—intravenous anesthetics like propofol or pentobarbital enter the protocol with ICU-level oversight outlined explicitly in this guide.
Each intervention demands precision: titration based on clinical response rather than rigid schedules ensures patient safety while maximizing efficacy—a balance deeply explored in this comprehensive pdf resource on Status Epilepticus Management Pdf.
The Role of Critical Care Monitoring and Post-Epileptic Care
Beyond acute control lies extended vigilance—a principle underscored throughout this Status Epilepticus Management Pdf framework. Patients emerging from prolonged seizures often suffer metabolic derangements requiring correction: hyperglycemia mitigation, electrolyte repletion (especially magnesium and potassium), acidosis management through bicarbonate if indicated. Early neuroprotective strategies including normothermia maintenance prevent secondary insults often overlooked in emergency phases but crucial for long-term outcomes.
Neurological assessment must extend beyond seizure cessation to monitor for coma progression or recurrent disconversion—a known trigger for secondary status epilepticus requiring renewed intervention cycles. The pdf stresses multidisciplinary coordination involving neurology, critical care nursing teams, and pharmacy support to ensure medication adherence and avoid polypharmacy pitfalls that may potentiate CNS depression or drug interactions during recovery phases.
Emotional support for caregivers forms an underrecognized pillar discussed here—not only physical recovery but psychological aftermath demands structured follow-up planning embedded within discharge instructions outlined alongside medical protocols in this PDF.
Concluding this essential exploration reveals that Status Epilepticus Management Pdf is not merely a procedural manual but a dynamic bridge connecting theory with real-world application under pressure. Its layered structure supports rapid retrieval during chaos while offering depth for ongoing education across clinical settings—from emergency rooms to intensive care units—ensuring providers navigate uncertainty with confidence backed by evidence-based guidance every step of the way.