Management of Hyperkalemia in Dialysis Patients: Essential PDF Guide
Management Of Hyperkalemia In Dialysis Patients Pdf serves as a vital resource for clinicians navigating the complex challenges of electrolyte control in renal failure. As potassium levels rise dangerously in patients undergoing dialysis, timely intervention becomes essential to prevent life-threatening arrhythmias and neuromuscular complications. This comprehensive PDF guide consolidates current best practices, evidence-based protocols, and practical insights into managing hyperkalemia effectively within the dialysis setting.
Understanding Hyperkalemia Risks in Dialysis Patients
Hyperkalemia presents a persistent threat to dialysis patients due to impaired kidney function and fluid shifts during treatment. The kidneys’ diminished ability to excrete potassium disrupts balance, while dialysis itself introduces variables like membrane permeability and dialysate composition that influence potassium removal. Patients often face multiple triggers—medications such as ACE inhibitors or potassium-sparing diuretics, dietary intake exceeding limits, or metabolic acidosis—each demanding vigilant monitoring and responsive care. Effective management hinges on recognizing these triggers early and integrating them into individualized treatment plans.
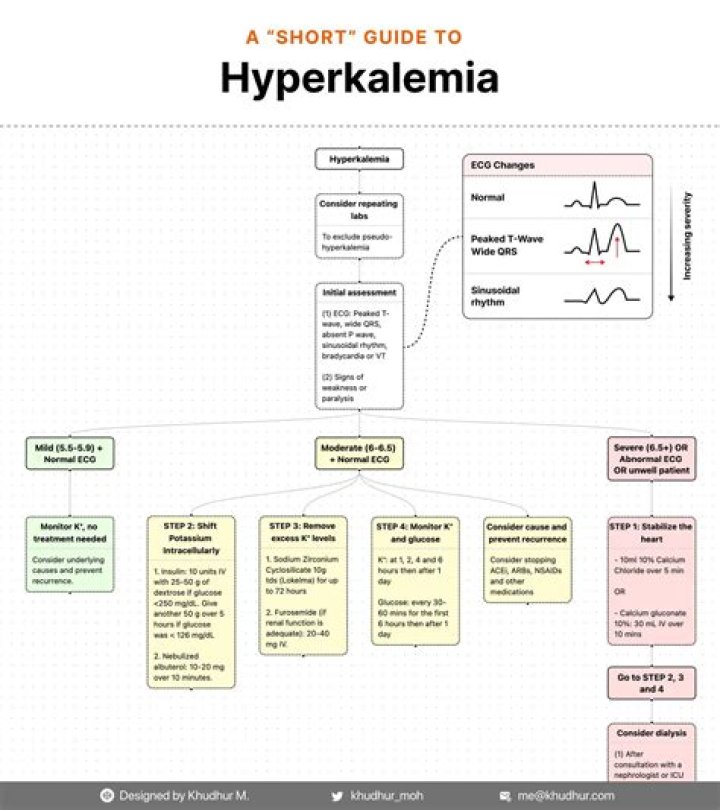
The Management Of Hyperkalemia In Dialysis Patients Pdf outlines a structured approach beginning with accurate assessment. Serum potassium levels must be interpreted within clinical context, factoring in ECG changes, muscle strength, and symptoms such as palpitations or paresthesia. Serial monitoring guides decisions on immediate interventions versus long-term adjustments. This section emphasizes the importance of consistent lab tracking and real-time data analysis to anticipate dangerous spikes before they escalate.
When acute hyperkalemia emerges during or between sessions, rapid action is paramount. Intravenous calcium gluconate stabilizes cardiac membranes without lowering potassium—it buys critical time while other measures take effect. Insulin-glucose infusions enhance cellular uptake of potassium, shifting it from blood into cells; sodium bicarbonate may correct acidosis, further promoting intracellular movement. These treatments are most effective when paired with careful fluid balance management to avoid volume overload or dehydration.
Long-term control centers on patient education and medication optimization. Dietary guidance remains foundational—limiting high-potassium foods like bananas, oranges, potatoes, and tomatoes—while tailored phosphate binders prevent secondary complications such as hyperkalemic periodic paralysis. Pharmacologic choices demand precision: spironolactone should be avoided if renal clearance is compromised; newer agents like patiromer offer alternatives with lower risk profiles. Adjusting dialysate potassium concentration emerges as a key modifiable factor; lowering it can reduce peak serum levels without sacrificing dialytic efficacy.
The PDF stresses multidisciplinary collaboration: nephrologists coordinating with dietitians ensures patients receive realistic dietary advice; nurses play a frontline role in vigilant observation for early warning signs; pharmacists assist in reviewing polypharmacy risks that may exacerbate hyperkalemia. Shared decision-making fosters adherence and improves outcomes across diverse clinical settings.
The Management Of Hyperkalemia In Dialysis Patients Pdf also addresses special scenarios—hemodialysis versus peritoneal dialysis differences influence timing and potency of interventions; acute kidney injury episodes require urgent recalibration of treatment algorithms; elderly patients face heightened vulnerability due to comorbidities and altered physiology requiring gentler management strategies.
Consistency remains the cornerstone of care:. Daily lab reviews reinforce pattern recognition; simulation drills prepare teams for rapid response; documentation standards ensure continuity across shifts. Each step in this process strengthens resilience against hyperkalemic emergencies.
Conclusion: Managing hyperkalemia in dialysis patients is not merely reactive—it demands proactive integration of clinical judgment, patient-centered strategies, and evolving evidence captured in resources like the Management Of Hyperkalemia In Dialysis Patients Pdf PDF guide. By combining precise diagnostics with compassionate follow-up, healthcare providers can significantly reduce morbidity and mortality tied to this common yet perilous complication.