Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension: Expert PDF Guide
Early Restrictive or Liberal Fluid Management for Sepsis-induced Hypotension Pdf offers a critical framework for navigating one of the most challenging clinical scenarios in critical care—managing blood pressure instability during sepsis. Sepsis-induced hypotension disrupts hemodynamic stability, demanding precise fluid strategies that balance volume expansion with risk of fluid overload. Understanding when to restrict or liberally administer fluids can mean the difference between recovery and organ failure.
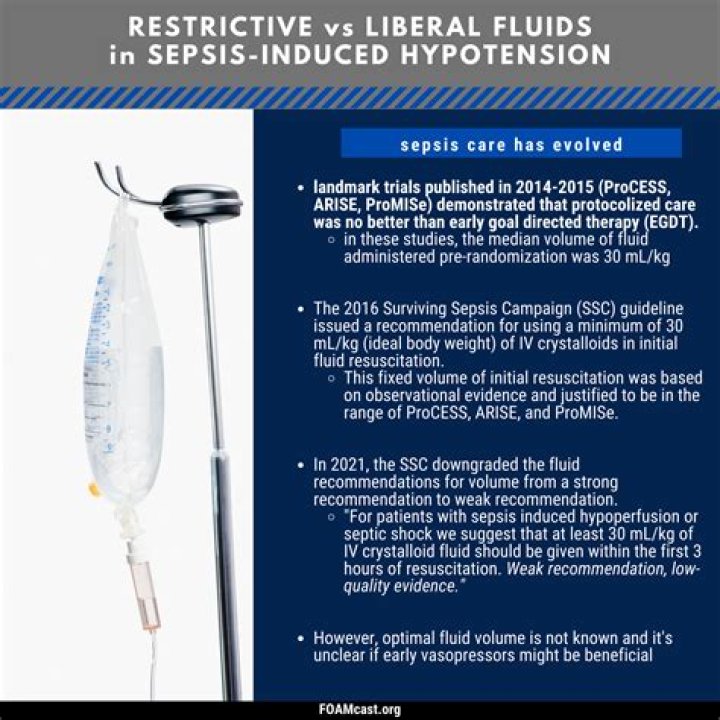
Navigating Fluid Strategies in Sepsis: A Deep Dive
Sepsis triggers a cascade of inflammatory responses, leading to vasodilation, capillary leak, and intravascular volume depletion—key contributors to hypotension. Early intervention with fluids remains central, yet optimal management hinges on careful assessment of patient physiology. The debate between early restrictive versus liberal fluid resuscitation reflects evolving clinical evidence and practical experience. Early restrictive approaches prioritize limiting initial fluid boluses to avoid complications like pulmonary edema while closely monitoring hemodynamic markers. Conversely, liberal strategies advocate aggressive initial infusion to stabilize blood pressure rapidly, especially in hemodynamically unstable patients. Both methods require integration within a dynamic early Restrictive or Liberal Fluid Management for Sepsis-induced Hypotension Pdf framework.
In this PDF guide, clinicians learn to tailor fluid administration based on real-time parameters: central venous pressure trends, lactate clearance, urine output, and response to initial boluses. Restrictive strategies often emphasize titrated infusions guided by invasive monitoring when available, while liberal protocols rely on rapid assessment and aggressive but cautious expansion. The choice isn’t binary; it depends on patient-specific factors including comorbidities, stage of illness, and organ dysfunction. Emerging data suggest hybrid models—combining restraint with responsive titration—may optimize outcomes by maintaining perfusion without overwhelming circulatory capacity.
The PDF underscores the importance of individualized care over rigid protocols. Early intervention is essential but must be balanced with vigilant monitoring for signs of fluid overload such as rising pulmonary pressures or worsening organ function. Point-of-care ultrasound and dynamic indices like stroke volume variation enhance decision-making beyond static metrics. Educating teams on recognizing early hypotensive thresholds enables timely adaptation—critical when managing sepsis-induced hypotension before irreversible damage occurs.
Conclusion The guide emphasizes that early restrictive or liberal fluid management for sepsis-induced hypotension Pdf is not about dogma but adaptive precision. By integrating clinical judgment with evidence-based algorithms embedded in this PDF resource, clinicians can navigate the delicate balance between under-resuscitation and overload. Mastery lies in continuous reassessment and responsiveness—ensuring every drop supports survival without compromise. This expert PDF stands as a vital tool for intensivists striving to optimize hemodynamic stability amid the chaos of sepsis.