Anaesthesia Management for Congenital Diaphragmatic Hernia: Essential PDF Guidelines
Anaesthesia Management of Congenital Diaphragmatic Hernia Pdf outlines critical strategies for ensuring safe and effective airway control during complex surgical interventions in affected infants. This PDF serves as a vital reference for anesthetists navigating the unique physiological challenges presented by congenital diaphragmatic hernia, a condition requiring meticulous perioperative planning.
The Role of Preoperative Assessment in Anaesthesia Planning
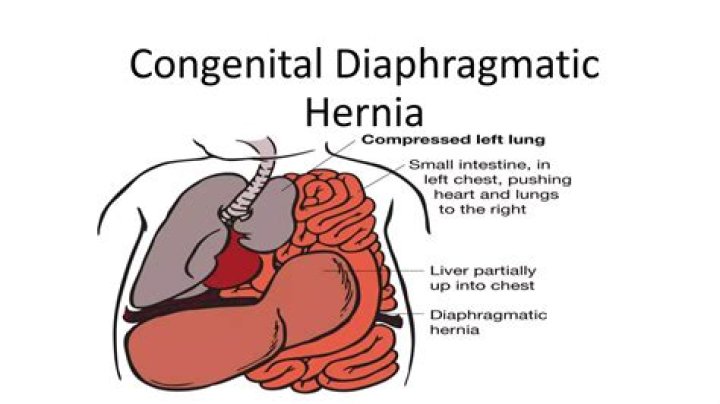
Understanding the anatomical disruptions caused by congenital diaphragmatic hernia is foundational to effective anaesthesia management. Preoperative evaluation must include detailed imaging, pulmonary function testing, and cardiac assessment to identify associated anomalies such as lung hypoplasia or cardiac malformations. These insights guide tailored anaesthetic protocols that minimize risks during intubation and mechanical ventilation. A thorough review of patient history reveals common comorbidities, including chromosomal disorders or syndromic associations, which significantly influence anaesthetic choices. Close collaboration with paediatric surgeons and intensivists ensures alignment on timing and approach, especially when considering staged repairs or emergency interventions. The PDF emphasizes early stabilisation of respiratory status, often requiring non-invasive ventilation preoperatively to reduce lung injury risk. Careful selection of muscle relaxants prevents prolonged paralysis while maintaining adequate muscle relaxation during surgery.
Airway Management: Balancing Safety and Efficiency
Managing the airway in infants with congenital diaphragmatic hernia presents unique challenges due to limited neck mobility and potential spinal instability. Traditional endotracheal intubation demands skillful technique, often using flexible bronchoscopy guidance when direct laryngoscopy is unfeasible. The PDF recommends securing the airway with minimal manipulation to avoid exacerbating diaphragmatic displacement. Cricoid pressure may be cautiously applied in selected cases but must be used judiciously to prevent airway compromise. Endotracheal tube selection prioritizes size appropriate for small infant anatomy, reducing the risk of tube misplacement or trauma. Continuous capnography and pulse oximetry remain essential monitoring tools throughout the procedure. In cases where conventional intubation fails, emergent surgical airway access via cricothyrotomy is outlined as a life-saving option—emphasized clearly in this comprehensive PDF guide.
Perioperative Anaesthetic Techniques
Anaesthesia management must integrate fluid dynamics carefully; hypovolaemia risks are heightened due to compromised pulmonary vascular resistance. Goals include maintaining stable preload without overloading fragile lungs, often achieved through conservative fluid administration guided by dynamic parameters like pulse pressure variation. Temperature regulation is paramount—hypothermia accelerates coagulopathy and impairs immune function in these vulnerable patients. Active warming strategies are strongly recommended during all phases of care. Analgesia regimens combine regional techniques with systemic opioids or non-opioid adjuvants to ensure comfort while preserving respiratory drive post-operatively. The PDF stresses avoiding volatile agents with prolonged pulmonary half-lives, favouring agents that allow rapid recovery without residual depression—key for early extubation readiness when indicated.
Postoperative Considerations
Recovery from anaesthesia demands vigilant monitoring for respiratory depression and autonomic instability common after diaphragmatic repair procedures. Early extubation protocols are supported if airway integrity is confirmed through clinical exam and capnography trends—both emphasized in this resource as essential checkpoints. Pain management remains critical; multimodal strategies reduce opioid reliance while preventing inadequate analgesia that could compromise respiratory effort or trigger self-extubation attempts in pediatric patients prone to agitation post-surgery. Close coordination with postoperative ICU teams ensures continuity of care aligned with anesthetic goals outlined earlier. This comprehensive guide underscores that effective anaesthesia management hinges on integrating anatomical insight with precise pharmacological control—ensuring optimal outcomes for infants living with congenital diaphragmatic hernia through structured knowledge captured clearly in the Anaesthesia Management Of Congenital Diaphragmatic Hernia Pdf resource.